
Difference between depression and hypoarousal?
Reading Time 4 mins

Imagine waking up on a grey Tuesday morning, looking at your alarm clock, and feeling an absolute, crushing weight pinning you to the mattress. The simple act of swinging your legs out of bed and walking to the kettle feels like attempting an unsupported trek across the Antarctic.
Your emotional landscape is completely flat, your mind is blanketed in a dense, unyielding fog, and you feel profoundly disconnected from the world outside your window.
If you were to consult a standard mental health checklist or look at your reflection through a conventional psychological lens, you would likely stamp a definitive label on this experience: clinical depression.
For decades, both traditional medicine and public health campaigns have taught us that any prolonged state of low energy, emotional numbness, and cognitive slowing is a definitive symptom of a depressive disorder.
However, as the fields of quantum biology, neuroscience, and somatic psychology have advanced, clinicians have uncovered a fascinating, highly critical alternative explanation.
You might not actually be depressed at all. Instead, your nervous system might simply be trapped in a physiological state known as hypoarousal.
While depression and hypoarousal look like identical twins on the surface, they originate from entirely different neighbourhoods of your biology.
Confusing the two is one of the most common pitfalls in modern wellness—and treating hypoarousal with tools designed for clinical depression can accidentally leave your nervous system feeling even more unsafe.
Here is the essential clinical breakdown of how to tell the difference between a psychological depressive state and a physiological autonomic shutdown, how the two can dangerously intertwine, and why that distinction completely reconfigures your path back to vibrant health.
The Core Distinction: Top-Down vs. Bottom-Up
To accurately separate these two states, we have to look at the direction the traffic is flowing through your nervous system.
Clinical depression is primarily a "top-down" phenomenon. It is deeply intertwined with the cognitive structures of the brain—the prefrontal cortex and the limbic system.
Depression is heavily anchored in complex mental architecture: a persistent loop of negative self-talk, historical rumination, stories about personal failure, and a psychological belief that the future holds no value.
The heavy physical exhaustion of depression is frequently the result of the mind being completely worn out by its own internal warfare.
Hypoarousal, on the other hand, is a strictly "bottom-up" survival mechanism. It is governed entirely by the oldest, most primitive portion of your autonomic nervous system: the dorsal vagal pathway of the vagus nerve.
Hypoarousal does not care about your thoughts, your childhood, or your philosophy on life. It is an instinctive, automated biological circuit that triggers when your brainstem decides that your system has run out of resources to fight off environmental stress.
To keep you alive, the brainstem pulls the master brake, plunging your body into an energetic freeze state. The numbness of hypoarousal isn't a psychological choice; it is an immediate physical reality.
The Symptom Matrix: Spotting the Biological Clues
Because these states present so similarly, we have to become biological detectives, looking closely at the subtle nuances of our daily symptoms to find out where our system is genuinely sitting.
1. The Role of the Inner Critic
In Depression: The inner voice is incredibly loud, sharp, and highly articulate.
It relentlessly tells stories about your inadequacies, deconstructs past mistakes, and generates profound feelings of guilt, shame, and unworthiness. The focus is psychological: "I am failing, I am a burden, nothing will ever change."
In Hypoarousal: The inner critic is remarkably quiet because your cognitive centres are simply offline.
There is no active internal narrative or complex story; there is just a vast, hollow emptiness. If you ask someone in hypoarousal what they are thinking about, the genuine answer is usually: "Nothing. My brain is completely blank."
2. The Nature of the Exhaustion
In Depression: The fatigue is often deeply tied to motivation and meaning.
You might have the physical strength to go for a walk or complete a project, but you are entirely missing the psychological drive or chemical reward (dopamine) to make it feel worthwhile. It is an absence of desire.
In Hypoarousal: The fatigue is absolute, chemical, and structural.
Your heart rate slows, your blood pressure drops, and cellular metabolism actively downregulates to conserve power. Your limbs literally feel like iron bars because your nervous system has temporarily restricted the energy flowing to your muscular architecture. It is an absence of physical capacity.
3. The Onset and Timeline
In Depression: The state typically materialises gradually over weeks or months, often linked to prolonged life transitions, grief, historical patterns, or seasonal changes. It behaves like a slow-moving weather system settling over your entire life.
In Hypoarousal: The descent can happen within a matter of minutes or hours. It often follows a specific, identifiable spike of acute over-stimulation, an intense conflict, or a prolonged period of frantic sympathetic hustle (the classic hyperarousal ceiling).
Your system suddenly hits its absolute limit, trips the circuit breaker, and drops you straight into the basement to protect you from burning out completely.
The Biological Bridge: How Hypoarousal Triggers True Depression
While it is clinically vital to separate these two states, we must also understand how they can form a dangerous biological alliance.
If your nervous system remains trapped below the floorboards of your Window of Tolerance for too long, a purely physical freeze state will actively trigger psychological clinical depression. This occurs through three distinct biological pathways:
1. The Brain's Narrative Trap
The human brain is a masterful storyteller that absolutely detests mystery; it is constantly monitoring your internal physiological baseline.
When you are stuck in hypoarousal, your brainstem forces a low-metabolic state—your posture collapses, your energy vanishes, and an emotional numbness sets in.
Your conscious mind notices this physical collapse and demands an immediate explanation. Because it does not inherently understand the language of the vagus nerve, it invents a psychological narrative to match the physical heaviness:
The Body feels: Heavy, immobile, and empty.
The Brain concludes:"I must be failing. My life is pointless. I am completely stuck."
Over time, this continuous loop transforms a temporary, protective physical freeze into a deeply ingrained psychological belief system.
2. Neurotransmitter Down-Regulation
During a prolonged dorsal vagal shutdown, your biology prioritises immediate organ survival over emotional thriving.
To save energy, the system sharply down-regulates the production and transmission of your "seeking and reward" neurotransmitters, primarily dopamine and serotonin.
Dopamine provides the exploratory drive to innovate, step outside, and tackle new projects, while serotonin maintains your baseline sense of ambient wellbeing.
When these chemical taps are turned off by a frozen nervous system, you lose the biological capacity to experience pleasure or motivation (anhedonia), driving you straight into a true clinical depressive cycle.
3. The Isolation Feedback Loop
Hypoarousal enforces a primitive, urgent behavioural impulse: to hide, pull the blinds, and isolate yourself from any environment that could further drain your energy.
While this isolation provides short-term shelter to an overwhelmed nervous system, long-term isolation starves the brain of positive environmental stimulation, social mirroring, and connection.
This enforced loneliness feeds a profound sense of helplessness and despair, cementing the psychological architecture of depression.
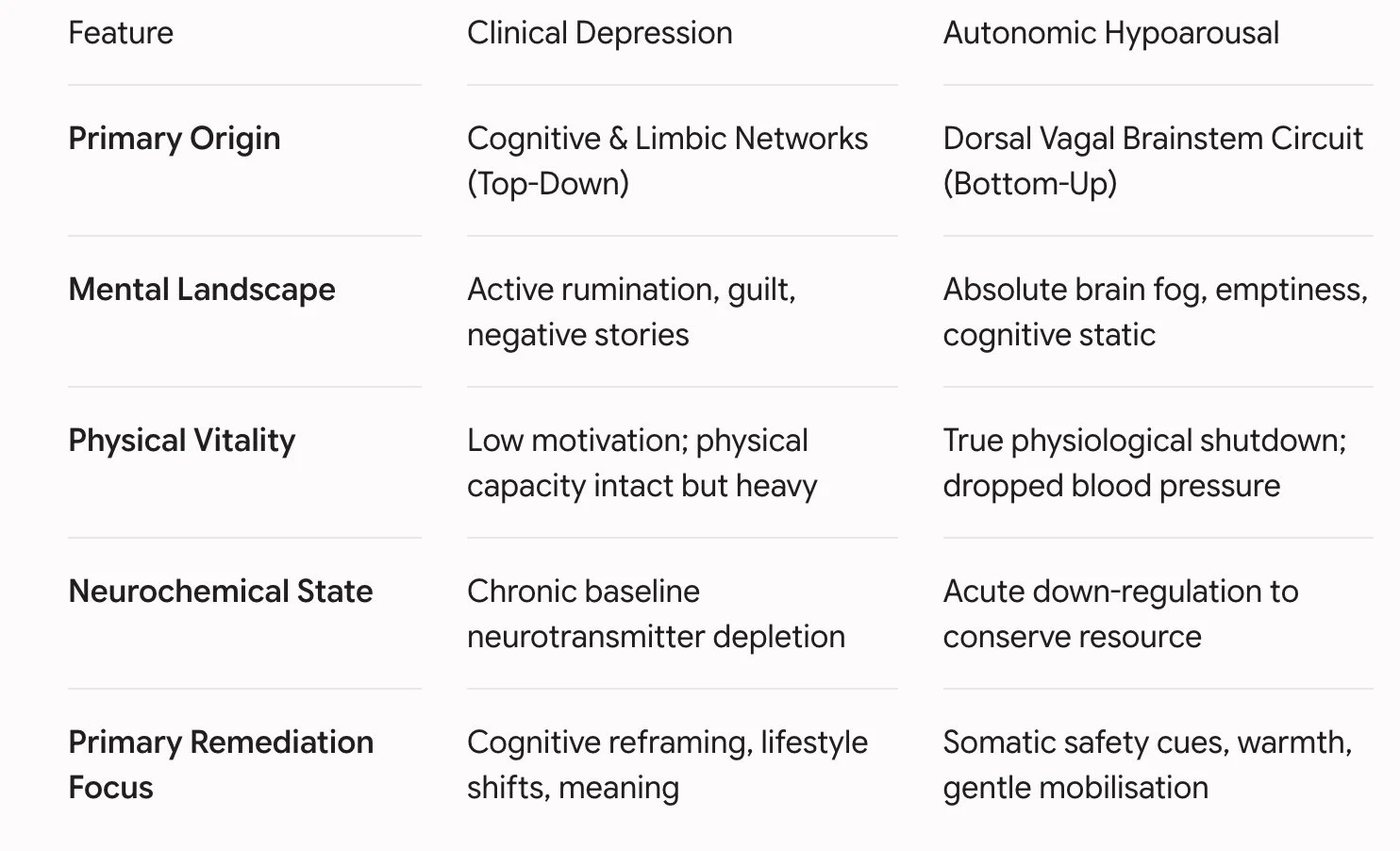
Tracking the Differences
To visualising how these states diverge and interact in daily operation, it helps to map their distinct characteristics side by side:
Why Misdiagnosis Matters: The Danger of the Wrong Remedy
Distinguishing between these two states isn't just an academic exercise—it is a critical operational safety measure for your health.
If you treat clinical depression with traditional top-down therapies—such as intensive cognitive behavioural analysis or forcing yourself to logically reframe your thoughts—you can make great strides in changing your mental landscape.
But if you apply those exact same tools to a body trapped in hypoarousal, you will often find yourself crashing even harder. When your system is in a dorsal vagal freeze, your brainstem perceives intensive mental analysis or harsh, forced discipline as a brand-new threat.
Forcing an already exhausted, shut-down body to "push through" or "think positive" simply sends a clear signal to your neuroception radar that you are still in danger, locking the basement doors from the inside and accelerating the slide into depression.
Conclusion: Honouring the System’s Wisdom
Whether you are navigating a season of true depression or a temporary state of autonomic hypoarousal, the ultimate path to recovery begins by dropping all judgment. Neither state represents a lack of willpower, a broken personality, or a personal failure.
If you discover that your low mood is actually being driven from the bottom up by hypoarousal, you can completely reframe your recovery. Instead of asking yourself, "Why can't I just be happier?", you can ask the far more useful, somatic question: "What does my body need right now to feel completely safe?"
By feeding your system slow, deliberate somatic cues of safety—gentle compression, warm environments, quiet spaces, and soft, supportive human connection—you can gradually convince your primitive brainstem that the crisis has passed.
Treat your biology with the grace and scientific understanding it deserves, and your nervous system will naturally release its defensive grip, gently lifting you out of the ice zone and back into a life lived with warmth, vitality, and unshakeable clarity.
Klarer M, Arnold M, Günther L, Winter C, Langhans W, Meyer U. Gut vagal afferents differentially modulate innate anxiety and learned fear. J Neurosci. 2014 May 21;34(21):7067-76. doi: 10.1523/JNEUROSCI.0252-14.2014. PMID: 24849343; PMCID: PMC6608191. https://pubmed.ncbi.nlm.nih.gov/24849343/
Lanius, R. A., Vermetten, E., & Pain, C. (2010). The impact of early life trauma on health and disease: The hidden epidemic. https://assets.cambridge.org/97805218/80268/frontmatter/9780521880268_frontmatter.pdf
McEwen BS. Physiology and neurobiology of stress and adaptation: central role of the brain. Physiol Rev. 2007 Jul;87(3):873-904. doi: 10.1152/physrev.00041.2006. PMID: 17615391. https://pubmed.ncbi.nlm.nih.gov/17615391/
van der Kolk BA. Clinical implications of neuroscience research in PTSD. Ann N Y Acad Sci. 2006 Jul;1071:277-93. doi: 10.1196/annals.1364.022. PMID: 16891578. https://pubmed.ncbi.nlm.nih.gov/16891578/
Read This Next






Disclaimer: This article is for general informational purposes only and does not address individual circumstances, substitute for professional advice, or serve as a basis for decision-making. You should always seek the guidance of a physician or qualified healthcare provider regarding a medical condition, and never disregard or delay seeking professional medical advice due to this content. Any action taken based on this information is entirely at your own risk and responsibility; Energetics, its staff, and its medical advisors disclaim all liability for any inaccuracies, errors, or any personal or professional loss incurred as a direct or indirect consequence of using this content.